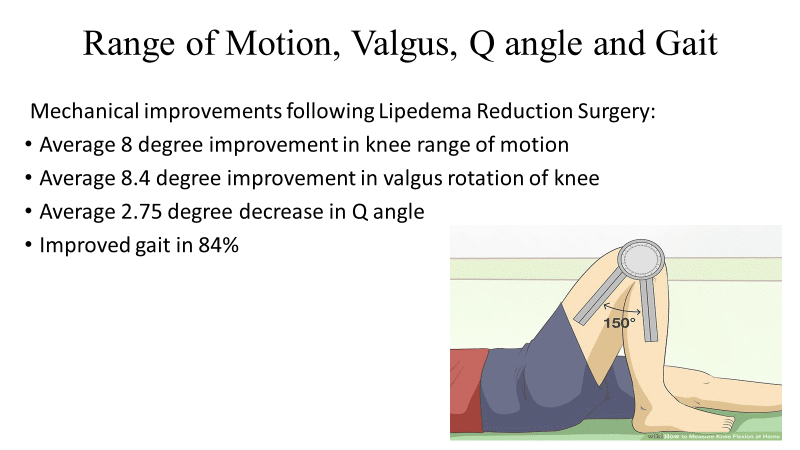
The disproportionate fat accumulation in Lipedema causes mechanical imbalances that result in significant orthopedic problems. Knee joint degeneration is the most common arthritic condition of lipedema patients and is often disabling. In our experience over the last five years, we’ve documented knee mechanics, including the range of motion, flexion, gait, q-angle, and knee joint angulation (varus or valgus) in the joint. We found that lipedema reduction surgeries have improved knee flexion by 8 degrees. That can make the difference between somebody being able to climb stairs, get in and out of a tub, or get in and out of chairs. Needless to say, this can be a huge difference! We’ve also seen about 8 degrees in valgus knee rotation, which evens out the pressure on the knee joint. As a result, this allows knee joints to last longer, avoiding arthritis that can result from rotation. Overall, 84% of patients who undergo lipedema reduction surgery over the 4-5 years had improvement in their gait and mobility, leading to more accessible and enjoyable lives. Read our full study here, and find more information on lipedema reduction surgery here.
I am grateful for Dr. Josef Stutz’s previous work on this subject. He has previously published a paper on the abnormal accumulation of fat in the inner thighs leading to a valgus deformity of the knee [knock knee], which puts increased pressure on the lateral knee compartment and leads to accelerating knee joint degeneration.
My talk focuses more on the fat accumulation in the distal thigh and proximal calf, causing a significantly restricted range of motion. The restricted range of motion and valgus deformity not only causes joint degeneration at the knee but also greatly complicates total knee replacement once the degeneration has occurred. Restricted range of motion and improper angulation of the knee joint are the number one and number two causes of failed knee replacement and chronic knee pain after knee replacement.
Objectives
- Identify how Lipedema can cause knee joint range of motion restrictions in patients with Lipedema.
- Explain how liposuction can improve a patient’s range of motion and mobility, decrease pain, and reduce stress on the knee joint.
- Describe how liposuction can improve postoperative recovery after joint replacement surgery – possibly even delay joint replacement surgery.
Patient Case Report
This is a case report of a lipedema patient who had an advanced degenerative joint disease of the knee with a markedly restricted range of motion.
Her orthopedic surgeon advised against proceeding with knee replacement because she would have a poor post-operative prognosis without correcting the abnormal fat deposits on her legs. Pre-operatively the patient’s range of motion was 88° of flexion. Normal flexion >130°.
KNEE ROM
Pain-Free / Mechanical Stress-Free
| Activity | Knee Flexion |
|---|---|
| Walking | 67° |
| Climbing Stairs | >90° |
| Descending Stairs | >100° |
| Sitting Down | 95° – 110° |
| Rising from Chair | 95° – 100° |
| Tying a Shoe | 105° |
| Squatting | 130° – 140° |
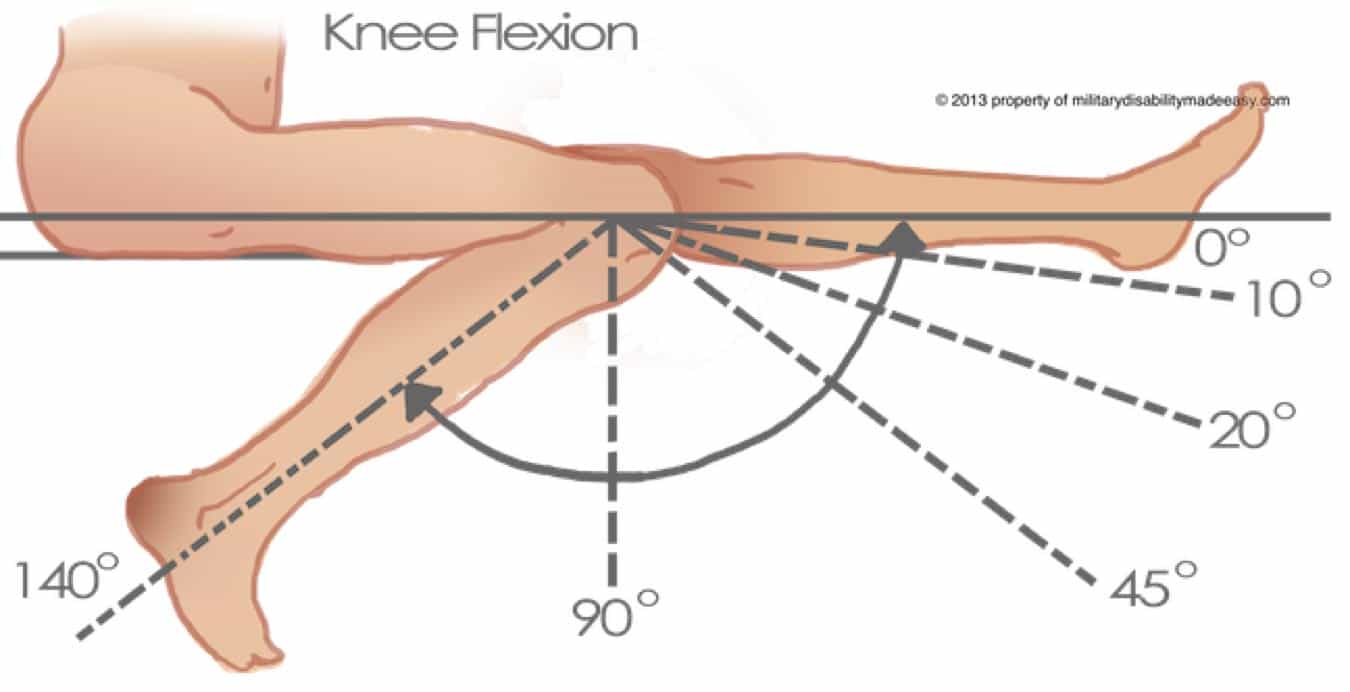
How We Measure Knee ROM & Knee Flexion
All these measurements are performed with a long arm goniometer following standard orthopedic exams. The ROM is flexion in degrees of rotation at the fulcrum of the knees measured by a long goniometer. The “pre” measurements are taken before surgery, and the post-measurements are taken at least six weeks after surgery.
Valgus is the deviation (or angulation) of the angle of the knee in the coronal plane. A typical knee is neutral, having no varus or valgus angulation. Same as above, pre is measured before and post is measured at least 6 weeks after surgery. This is caused by the spread of the legs from lipedema tissue and is associated with lateral tibiofemoral knee arthritis.
The Q-angle is measured by extending a line through the center of the patella to the anterior superior iliac spine and another line from the tibial tubercle through the center of the patella. Normal is 13-18 degrees. Deviation of over 18 degrees affects the patella tracking and is associated with knee pain, and may lead to degeneration of the patella cartilage.
Why are Knee ROM & Knee Flexion Measurements Important?
They show how lipedema affects the mobility of women. They show the concrete limitation that lipedema causes in leg function and how it affects the daily lives of women with lipedema.
Normal Range of Motion: No Lipedema
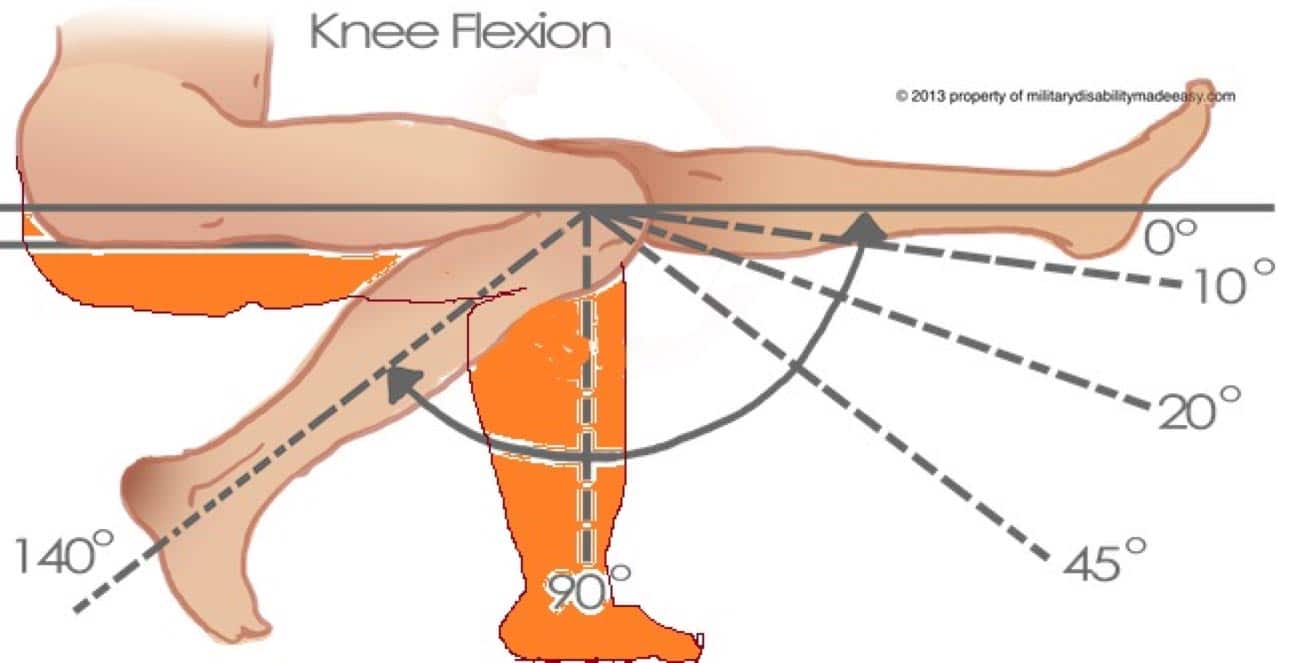
Restricted Range of Motion: With Lipedema
Post Operative Care
Post-operatively, after lymph-sparing liposuction, the patient had 120° of flexion and extension allowing for pain-free descent of stairs. The valgus angulation was corrected over 5°. The greatest improvement in pain came from her ability to rise from a chair and get out of the bathtub pain-free. Prior to the surgery, the patient experienced significant pain with these activities. However, the patient still had some pain with climbing stairs as the joint degeneration itself was not treated – just an improved range of motion.
Before & After
The removal of abnormal fat from the posterior thigh, anterior thigh to the knee, and from the upper calf, which restricted the flexion, significantly improved the patient’s knee mechanics. This has also improved mechanical joint stress with activity and greatly improved pain during activities of daily living (ADL). At a minimum, the patient has been able to postpone total knee replacement, and if she does eventually have a total knee replacement, the likelihood of a successful knee replacement is significantly increased
Liposuction to the legs significantly improved static and dynamic mechanics of the knee, decreased pain, increased patient mobility, and ability to carry out daily activities.
Can You Prevent Lipedema?
No, Lipedema cannot be prevented. Conservative methods such as diet and exercise may help to reduce inflammation, increase mobility, and prevent progression of the disease, but cannot prevent the disease from developing. Learn about your best natural options here.
Should I have a knee replacement or lipedema surgery first?
The decision to have knee or hip replacement surgery before or after lipedema surgery is an individual one and depends on the details of a person’s condition.
Factors to be considered include:
- Status of the joint that will be replaced and the extent to which joint issues are interfering with daily activities.
- Size, shape, and locations of lipedema fatty tissues that would be removed.
- In general, removing lipedema fat before joint replacement may provide a better outcome because:
- Lipedema tissue removal on the thighs can restore more normal limb positioning and reduce medial strain on the joint and help knee joint alignment. Lipedema tissue removal on the calf and thigh help the knee have more normal bending or range of motion. This improves the chance of successful knee replacement.
- Circulation will be improved after lipedema surgery to support faster healing.
References:
Dr. Josef Stutz, Liposuction of Lipedema to Prevent Later Joint Complications, Translated from Vasomed, Vol 23, January 2011
Wright, Thomas MD*; Babula, Megan AS*; Schwartz, Jaime MD†; Wright, Corbin BS, MS‡; Danesh, Noah BA†; Herbst, Karen MD, PhD†. Lipedema Reduction Surgery Improves Pain, Mobility, Physical Function, and Quality of Life: Case Series Report. Plastic & Reconstructive Surgery-Global Open 11(11):p e5436, November 2023. | DOI: 10.1097/GOX.0000000000005436