Getting an initial diagnosis for Lipedema is typically time-consuming, challenging, and emotionally draining. Why? Because the misdiagnosis starts from a very early age and comes from those closest to us, and even from the patient themselves. Those of us suffering from Lipedema commonly hear phrases like, “You’re just big-boned,” or, “You have a pear shape, it’s just your body.” Family members are quick to suggest that larger bodies or a specific body shape run in the family, and there’s not much we can do about it. While the assertion is harmless, it may not be the full truth. And while it’s normal for many women to accumulate fat in their thighs, hips, and buttocks, when is it beyond the normal range? When is it more than just “curvy”?
The typical explanations we hear in adolescence accelerate in adulthood. After years of trying every diet and exercise routine under the sun, many seek medical advice in the hopes of an explanation. This time, the common phrases range from “Maybe you need to control your appetite and portion sizes,” to, “I know you say you’re working out and have a balanced diet, but the scale says otherwise.” By the time we learn about Lipedema and make our way a specialist, we’ve been dismissed by other professionals, exhausted by our endless efforts, and worn down by the journey.
The question that ultimately leads us to a Lipedema diagnosis is a simple one which we are asking from childhood; “My legs look fat – Is that normal?” The mainstream answers and commonly accepted explanations are what lead us to constant frustration. If calories we take into our body equal calories we burn off, we “shouldn’t” be gaining weight, right? If the calories we take into our body are fewer than the calories we are burning, we should lose weight. Right? If this equation rings true, then why are my legs so different?
Weight Distribution
To answer this question, we must first ask several more. First, let’s evaluate how our legs may physically look different than other overweight body types. Do you tend to gain weight around the “trunk” of your body? For example, if you fold your body in half at the hips, would your bottom half be significantly larger and out of proportion with the top half? It’s common for women with Lipedema to report vastly different clothing sizes between their upper and lower bodies, such as wearing a size M or L shirt, but a size XXL in pants. For me, I’ve always had an extremely slim waist, so much so that my swimsuit tops were an extra small, and my bottoms were an XL. As much as I wanted to wear a one-piece to cover up as much as possible, there simply was not a size that existed to fit my extreme pear-shaped body. The shape of your legs and how you carry weight is also telling. Do your legs appear thick and column-like, without much definition or shape around the knees? This was a key feature of my body that ultimately led to my personal discovery of Lipedema.
Next, evaluate the effects of your weight gain on your ankles and feet. Do your feet appear to gain weight similar to the rest of your legs? Or, does the weight gain stop at the ankle, and your feet remain relatively “normal” in size? This may cause a cuff-like effect around the ankle as if you had a rope tightened around the bottom of your legs. If you’re like me, you might not be able to wear certain types of boots or shoes, because they either accentuate your cankles or they aren’t able to fit over your calves.
With Lipedema fat, we experience fat accumulation in specific areas, which may help indicate if your weight gain is normal or not. If you’re gaining pockets of fat that are out of proportion to other areas, this may be a tip-off that you have Lipedema. This can be difficult to catch because patients are often in the third stage of Lipedema when it becomes clear that the gains are irregular across the body. Here a few other areas of the body that can help determine if your weight gain may be due to Lipedema:
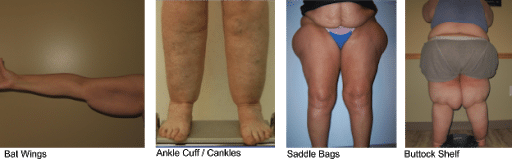
- Cankles: fat accumulation around the back of your ankles, causing an “ankle cuff.” This type of weight gain is a clinical sign only seen in Lipedema. Not all patients get this, but if you have it, it may be an indicator
- Bat Wings: Weight gain in your upper arms, causing a “bat win” effect. This is seen in about 80% of women with Lipedema.
- Saddle Bags: Large areas of fat that project outwardly beyond the normal curve of your hip, also known as “football saddle bags” (because they look like there’s a football on the sides of your hips).
- Buttock Self: This is a larger buttock that sticks out significantly from the lower back when looking at your silhouette from the side. This is another feature seen in most women with Lipedema.
Pain & Mobility Issues
In addition to the differences in physical appearance, women with Lipedema also commonly experience a range of painful symptoms. Do you bruise easily in the affected areas? For example, many patients report that they’ll get bruises from lightly bumping a chair, or may not know where their injuries came from at all. Additionally, do you feel pain from light touches to the affected areas? If your family pet jumps on you, or if your child grabs your leg, would this cause you pain? Typically, this bruising and sensitivity lead to an inability to remain physically active, further increasing weight gain.
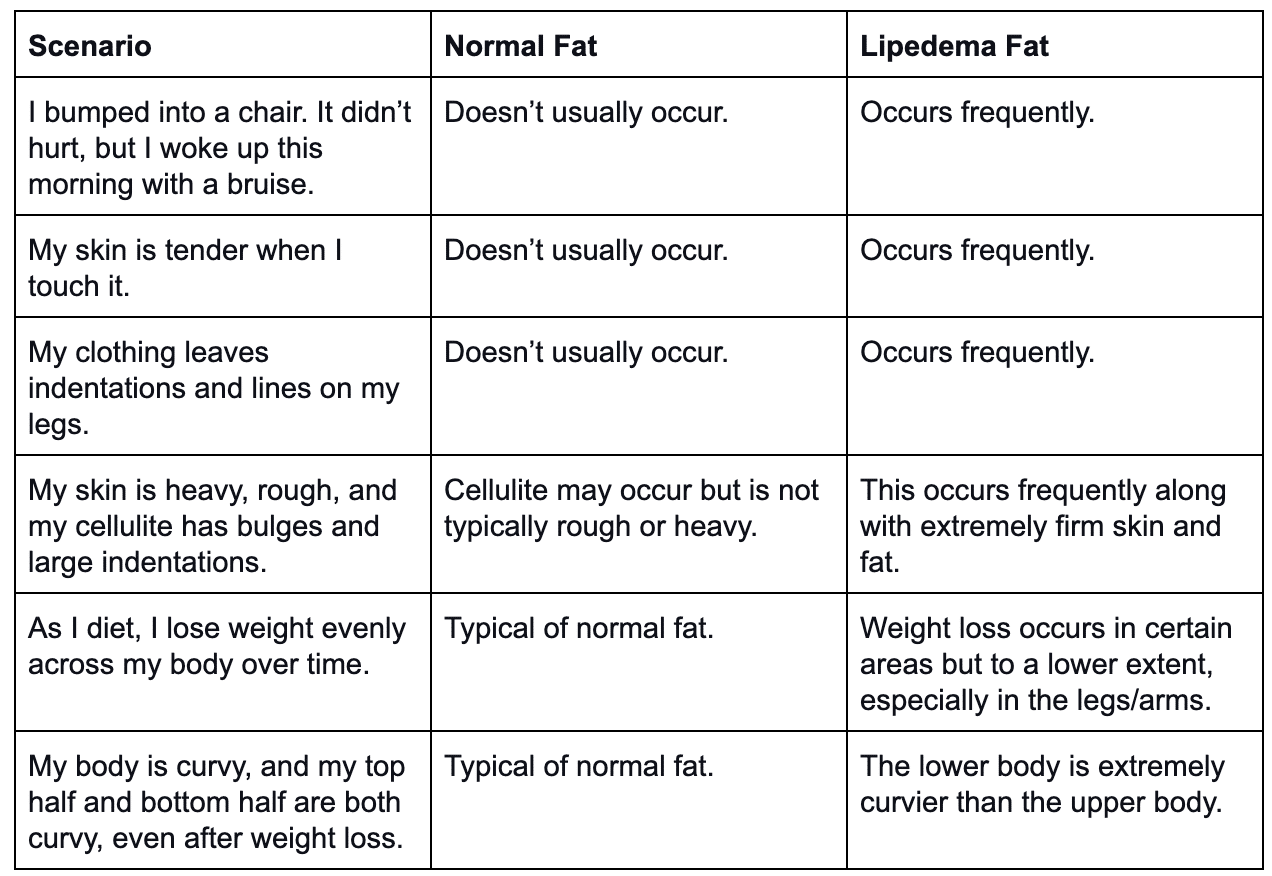
Normal Fat vs. Lipedema Fat
How do you determine what’s normal fat vs. Lipedema fat, and what’s a normal sensation versus an abnormality caused by Lipedema? This part can be difficult to determine, especially because many side effects aren’t detected until the later stages of Lipedema. So how can we catch this as early as possible? The table below offers a comparison of what’s widely experienced by women with Lipedema vs. what we usually see in normal fat or obesity.
Getting Real Answers
Getting a proper diagnosis is both time-consuming and challenging. The lack of awareness both in the medical community and in society as a whole makes it difficult to know when it’s appropriate to seek medical attention. Even then, because of the lack of awareness, your doctor may not recognize the symptoms as Lipedema. They may not be aware of the disorder at all. To add insult to injury, if they do realize it, they may not be trained on how to diagnose it or what the next steps should be. It’s important to advocate for your health, know the signs and symptoms, and seek out expert guidance.
This disease is a subcutaneous fat storage disorder that is not widely recognized by the medical community (yet). This disorder mainly affects women, causes an enlargement of the legs due to deposits of fat under the skin, and typically gets worse over time, making diagnosis and treatment essential.
While there may be a genetic component to Lipedema, the exact cause is not yet known. And while other fat disorders can cause many of the symptoms mentioned here (such as Dercum’s and Madelung’s disease), the majority of the time, the result is almost always a Lipedema diagnosis. Today, we know that Lipedema leads to an excessive build-up of fat cells, primarily in the lower body (although it can affect the arms and abdomen), and it disproportionately creates pockets of fat. The negative appearance of these cells is compounded by the physical pain and sensitivity that comes along it. While patients are frustrated and discouraged by the negative appearance of their legs, chronic pain is what drives them to continue seeking answers.
Sufferers experience easy bruising and tenderness, and pain in the affected areas. Patients overwhelmingly report being misdiagnosed by their families and doctors as being obese. Unfortunately, Lipedema fat is far more stubborn than regular fat, and will not respond to diet or exercise. Those with this disorder may workout regularly and practice healthy and balanced nutrition but will continue to gain weight. Or worse, they experience weight loss as the normal fat is lost, yet the painful, Lipedema fat remains. Commonly, the lack of effectiveness from a regular diet and exercise program is what prompts patients to recognize something isn’t right in their bodies. Even still, patients are often at odds with their doctors and are provided with solutions that do not address their underlying condition, ongoing pain, and consistent frustration. Unfortunately, it’s not uncommon for individuals with Lipedema to have more awareness of the disease and its treatment than the doctors and nurses who they encounter in their search for diagnosis and treatment.
How common is lipedema? Find out here.
Weight Loss and Lipedema
In 2019, I started training for a half-marathon and was running an average of 40 miles per week. During this time, I noticed that my upper body, arms, and face started to drop weight, but a strange fluid and fat mix around my thighs and knees just wouldn’t budge, no matter how healthy and active I was. My legs felt heavy and painful to move, and the only relief I found was wearing two pairs of workout pants to keep my legs as tight as possible. This was the turning point for me; How much more could I possibly do to get my body where it needed to be? After completing the half-marathon in April 2019, I started to aggressively look for answers. I was googling things like, “Why can’t I lose weight around my knees?” and “Why are my legs tender when I barely touch them?” I’ll never forget the moment I found a Reddit forum about Lipedema and how many are affected. This was the moment that changed my entire life.
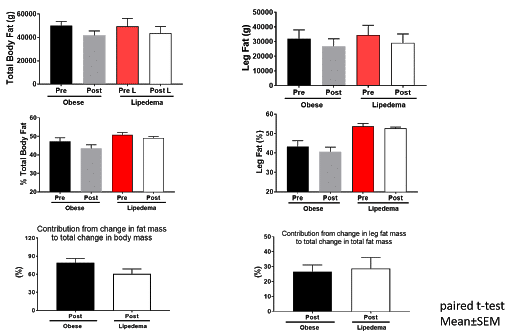
To further explore this frustrating aspect of Lipedema, a Washington University School of Medicine study evaluated the effect of diet-induced weight loss on body composition on both normally overweight patients and those who were overweight due to Lipedema. All participants were first properly diagnosed with Lipedema on their legs by ruling out other causes of legs swelling, such venous insufficiency. The study subjects received both a body composition scan with DEXA [Dual Absorption Xray] and an MRI to ensure an accurate baseline body composition evaluation. Each participant met with dietitians to create personalized healthy meal plans designed to achieve an 8-10% weight loss goal over the course of 6-8 months. All meals were prepared in the medical school metabolic kitchen and calories accurately counted. Afterward weight loss was achieved, each patient received the same body scan and MRI to determine how their body composition responded.
Each participant’s meal plan reduced their daily calories by 25% and included gluten, dairy, and egg-free meals as needed. They met with their dietitian weekly to record progress and pick-up food for the following week. The control group in this study went through the same process, however, they were diagnosed as obese and not with Lipedema, yet their BMI and age mirrored those in the Lipedema group.
For those of us struggling with Lipedema, the results of the study come to no surprise. While the group who had Lipedema was able to lose weight and decrease their body fat percentage, the decrease in percent body fat was lower for individuals with lipedema than those with classic obesity. Additionally, the post-weight loss body composition scans showed that the participants with Lipedema did not experience a significant loss of fat in their legs. So, while they did lose weight, their legs remained mostly the same. Those with classic obesity experienced higher weight loss, a greater decrease in their percent of body fat, and significant weight loss in their legs. Please note these 10% weight loss results are hard to translate into the real world. Unfortunately, in the real world we don’t have the luxury of someone preparing all of meals, counting calories, and coaching us weekly or more if needed along the way.
So Now What? Life After a Lipedema Diagnosis & Treatment
The only way I can fully explain learning about Lipedema is to explain it like a lightning bolt. In an instant, every moment of frustration, embarrassment, physical and emotional pain, and shame from my doctors were replaced with clarity – everything made sense now. I no longer was ashamed that I couldn’t figure out how to get my body to look like everyone else’s. Even before I found a specialist, I felt hopeful and excited for the first time in my life. Maybe I wasn’t a failure, I wasn’t crazy, and I wasn’t obese. Maybe I wasn’t alone in my struggle, and I could find something that would actually help! Fast forward exactly one year, and I’ve had two surgeries on my thighs, with plans to get three more. My thighs are nearly pain-free, I can go for long walks without feeling heavy and swollen, and I can play with my dog without getting bruised from her jumps. I’m experiencing life like I haven’t ever before. And the better I feel, the more I’m recognizing how much pain I was in for my entire life.
If you think you might have Lipedema, the first step is to see a doctor for a diagnosis. You can read more about the physical exam and necessary tests to determine if your provider can help you through this here. An ongoing treatment plan should be discussed with a medical professional, but you can read more about surgical options here, and non-surgical ways to live with Lipedema here. While there’s no cure for this disorder, a diagnosis is the first step to better understanding your body and, most importantly, that this is not your fault. The answer to your question, “Why are my legs so different?” is not that it runs in the family or that you aren’t doing your best. The answer is that you have Lipedema, and we’re here to help you through it.