Lipedema is an abnormality of the subcutaneous adipose [fat] tissue. Let me explain this a bit more. Adipose Tissue is the body principle structure for long term energy/calorie storage. But not all adipose tissue is the same. Still not sure what is lipedema fat and what is normal fat? Read on below.
There are four different kinds of adipose tissue. There is what I call essential adipose tissue which is the fat that is in your organs, bone marrow, and the like that is necessary for proper metabolic function. That is to say, there is a minimum amount of fat that is needed in organs like liver, kidney, and bone marrow for them to function properly.
The second type of adipose tissue is visceral fat. Visceral fat, which is the fat that is inside the abdominal cavity is the most metabolically active and sensitive fat depot to calorie balance changes. Visceral fat expands easily when there is excess calories and contracts when the body has a net calorie deficit.
The third fat depot is subcutaneous fat, the fat that is between the skin and muscle. This is the layer of fat attached to the underside of the skin or hypodermis, that is necessary to cushion our bodies and retain heat. It is less metabolically sensitive than visceral fat.
The fourth type of fat is hormone-dependent subcutaneous fat, also known as gynoid fat which is the fat that females accumulate and creates their secondary sexual characteristics. This is the fat that forms breast, hip, and inner thigh curves. It starts at puberty under the influence of estrogen and progesterone and is what gives the feminine shape to female’s bodies. This fourth fat depot is even less metabolically active than visceral or regular subcutaneous fat and this is the fat that is affected by lipedema.
New Insights Into Lipedema Fat Cells & Tissue tw ds 12_28_21 (1)
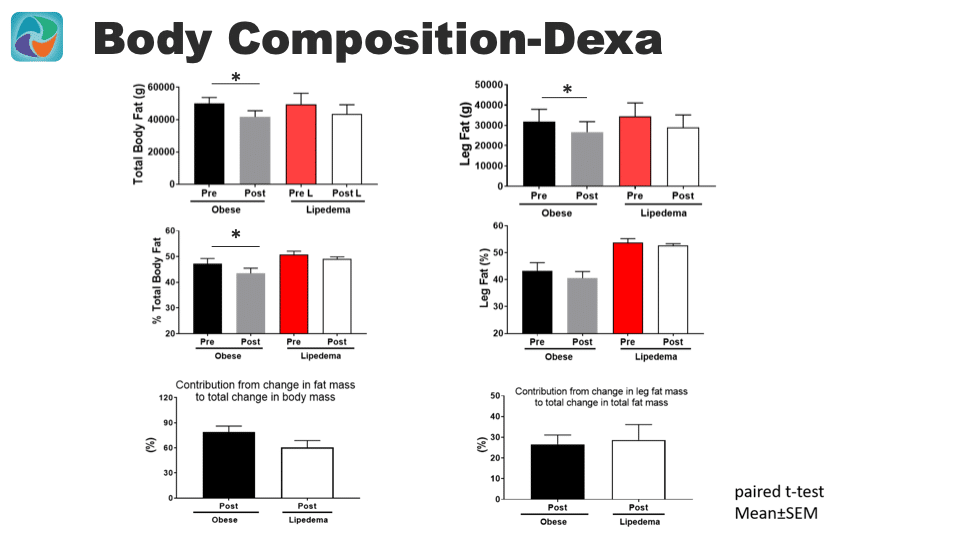
Changes in Body Fat Composition in Lipedema with Weight Loss
On the left side of the slide below, you can see graphs that show individuals with lipedema have a greater percentage of total body fat measured by DEXA scans compared to BMI matched individuals who meet the classical definition of obesity. The individuals with lipedema were able to lose weight and decrease the percent of total body fat. However, the change in percent of total body fat was significantly less in individuals with lipedema compared to BMI matched obese controls with weight loss. In other words, obese individuals with weight loss are able to significantly decrease their percent total body fat but lipedema individuals did not with the same amount of weight loss.
On the right side of the slide below, the graphs show the changes in leg fat measured by DEXA scans in classically obese compared to individuals with lipedema. The top right graph shows that both classically obese and individuals with lipedema lost fat in their legs. The decrease in fat was statistically significant in an individual with classical obesity. The percent of fat in the legs was not significantly changed in individuals with lipedema.
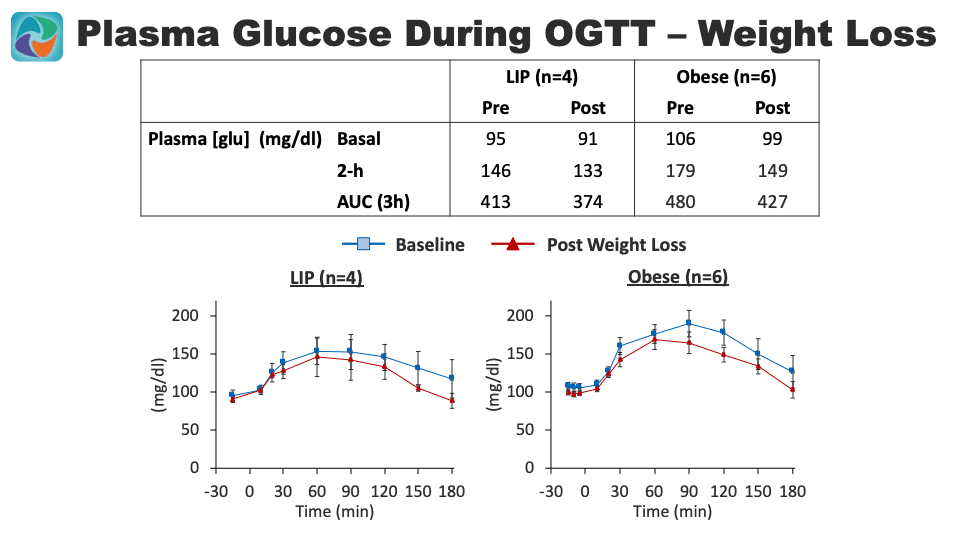
Changes in Plasma Glucose with Weight Loss in Lipedema.
The slide below shows graphs of fasting plasma glucose levels and after an Oral Glucose Tolerance Test (OGTT). Prior to weight loss, individuals with lipedema have a slightly lower fast blood sugar 95 compared to BMI matched classically obese individuals 106. The patients with lipedema also had lower blood sugars 2 hours after consuming a high glucose drink 146 compared to matched classically obese individuals 179. After weight loss, the lipedema patient’s blood sugars were lowered further. With weight loss, the obese matched individuals lowered and improved their blood sugars, but didn’t quite reach the level of lipedema individuals even prior to their weight loss.
What is Lipedema Fat? How is it Different from Normal Fat?
Lipedema is a disorder that affects the fourth depot of fat. Lipedema usually affects the arms and legs although in later stages it can spread to the rest of the body. The characteristic areas affected by lipedema are the thighs and hips. We don’t know why only certain areas of the body where the hormone-dependent subcutaneous fat exists are affected by lipedema, but for example, the breasts are not usually affected by lipedema early in the course of the disease.
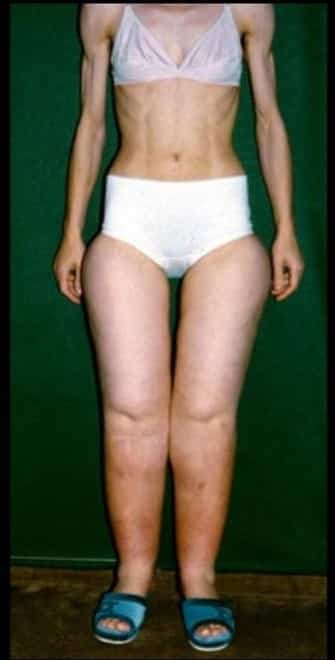
Lipedema fat is the least responsive to calorie balance deficits. In other words, this type of adipose tissue is very resistant to weight loss. This means that when weight loss occurs in a patient with lipedema, the other fat depots will be much more affected than the fat deposits where the lipedema exists. An individual will lose visceral fat and subcutaneous fat in areas not affected by lipedema, but very little fat in the lipedema affected areas.
To prove this point, I have attached a picture of a lady who is malnourished and underweight yet still has gynoid fat on her legs consistent with lipedema. This is the clearest visual example of the metabolic resistance of the fat of lipedema. We don’t know if the metabolic difference of lipedema fat is the cause of lipedema or it is the result of the change from lipedema but it is one hallmark of the diagnosis of lipedema.
NOTE: Lipedema is pronounced and spelled in several different ways. It is pronounced as lip-edema and lipo-edema – it can also be spelled lipedema, lipoedema, lipodema, and Lipödem. The spelling is all correct but one or two spellings are predominantly used in different countries.
We have had these clinical and surgical insights confirmed over the years, however, we have not known the detailed cellular and metabolic changes that create these differences explained sufficiently. This November of 2021 a very important paper studying the two key components of adipose tissue: Adipose Cells and their precursor’s cells Adipose-Derived Stem Cells ADSCs was published in International Journal of Obesity; https://doi.org/10.1038/s41366-021-01002-1.
In the paper Ishaq et al, report on their very sophisticated and elegant study of the differences of these cells in terms of their gene expressions, cellular components, metabolic products, mitotic rate, and propensity for proliferation. Further, they report on a possible gene that may play an important role in the development or perpetuation of lipedema, Bub1. This paper is a very important step in our understanding of the difference between subcutaneous loose connective tissue or adipose tissue of individuals with lipedema and those without lipedema. This study further solidifies the evidence that lipedema is a fat tissue disease and will further quiet the critics who confuse lipedema with lifestyle-induced obesity.
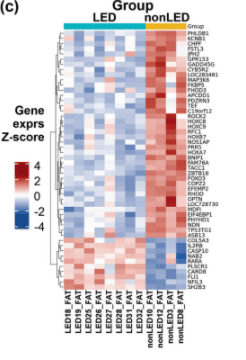
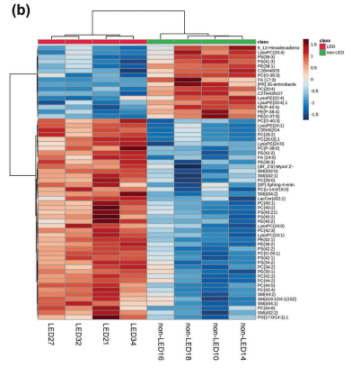
Lipedema adipose tissues show distinct gene signature [different genes are turned on].
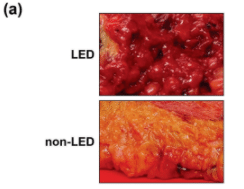
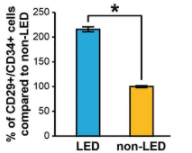
The stem cells from the lipedema fat show that the Adipose-Derived Stem Cells (ADSC) were greater in number compared to people without lipedema. Adipose-Derived Stem Cells (ADSC) are cells that can continuously divide and renew themselves and/or divide and become mature fat cells or other types of cells to sustain or grow fat tissue.
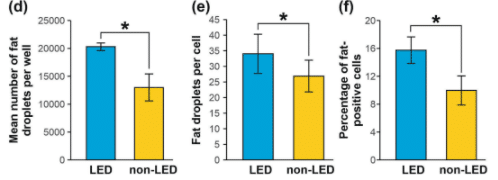
The number of fat droplets, percentage of fat-positive cells, and number of fat droplets/cells were significantly increased in lipedema adipocytes compared to controls. Lipedema fat cells had more fat in them.
Different lipid composition in fat cell of lipedema patients. The difference in lipid composition includes significantly increased lipids in lipedema included glycerophospholipids and sphingolipids.
Different metabolism of lipedema fat vs regular fat as characterized by differing production of Amino Acid and phospholipid production.
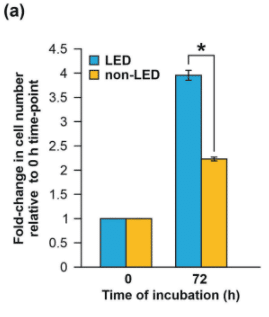
Adipose-Derived Stem Cells (ADSC) are cells from lipedema adipose tissue that display a hyperproliferative [increased rates of cell division and replication] state compared to those from BMI-matched patients.
Cell-cycle genes involved in regulating cell growth and proliferation are dysregulated in lipedema ADSCs and may contribute to the increased adipocyte number, and maldistribution and accumulation of dystrophic fat in lipedema.
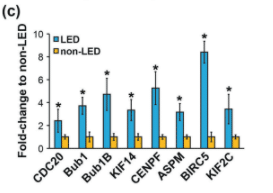
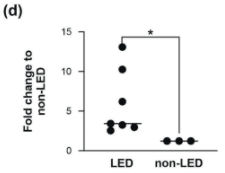
One gene called Bub1 is turned on more or upregulated in lipedema. [Bub1 mRNA production in ADSC from Lipedema compared to controls]. The Bub1 gene’s overexpression is associated with hyperproliferation and dysregulation of key cellular processes in several cancers. Ishaq et al. note that the overexpression of Bub1 in lipedema could play a similar role in hypertrophy ad persistence of lipedema fat tissue as it does in cancers such as gastric cancer.
Grabsch H, Takeno S, Parsons WJ, Pomjanski N, Boecking A, Gabbert HE, Mueller W. Overexpression of the mitotic checkpoint genes BUB1, BUBR1, and BUB3 in gastric cancer–association with tumour cell proliferation. J Pathol. 2003 May;200(1):16-22. doi: 10.1002/path.1324. PMID: 12692836. https://pubmed.
Lipedema: A Relatively Common Disease with Extremely Common Misconceptions Donald W. Buck, II, MD corresponding author* and Karen L. Herbst, MD, PhD† PMID: 27757353
Plast Reconstr Surg Glob Open. 2016 Sep; 4(9): e1043. Published online 2016 Sep 28. doi: 10.1097/GOX.0000000000001043. PMCID: PMC5055019